summary
Immune-mediated hemolytic anemia (IMHA) is a canine hemolytic disease caused by primary or secondary factors that lead to the animal's own red blood cells being incorrectly labeled by the immune system and thus being cleared in large quantities, resulting in severe anemia, jaundice, loss of appetite, and other symptoms. The mortality rate is as high as 80%.
This article will analyze and discuss the diagnostic approach for a dog with severe anemia caused by IMHA, providing diagnostic insights for clinicians when encountering anemia of unknown cause.
Keywords: Acute jaundice; Anemia; IMHA; Case report
01
Case Information
1.1 Animal Information
Male Schnauzer, 7 years and 1 month old, weighing 9.27 kg.
1.2 Chief Complaint
The dog was brought to the hospital for treatment due to loss of appetite. During the visit, it suddenly developed acute jaundice. After blood transfusion and hormone treatment proved ineffective, it was transferred to our hospital. The cause of the illness has not yet been determined.
1.3 Physical Examination
Weight 9.27 kg; body temperature 37.8°C; respiratory rate 24 breaths/min; heart rate 59 beats/min; BCS 5/9; mildly delayed skin elastin, CRT <2s; moist and jaundiced oral mucosa; no abnormalities found on abdominal palpation; no enlarged superficial lymph nodes.
1.4 Clinical Symptoms
The animal's skin and mucous membranes are jaundiced. The animal is in poor spirits, has no appetite, vomits, and has soy sauce-colored urine.
1.5 Diagnostic Plan
Anlu formed element blood analysis; biochemistry; Anlu formed element urine analysis; ultrasound; blood smear.
02 Inspection results
2.1 Complete Blood Count
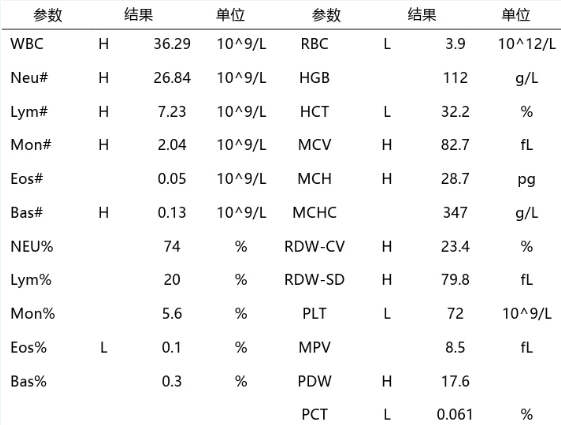
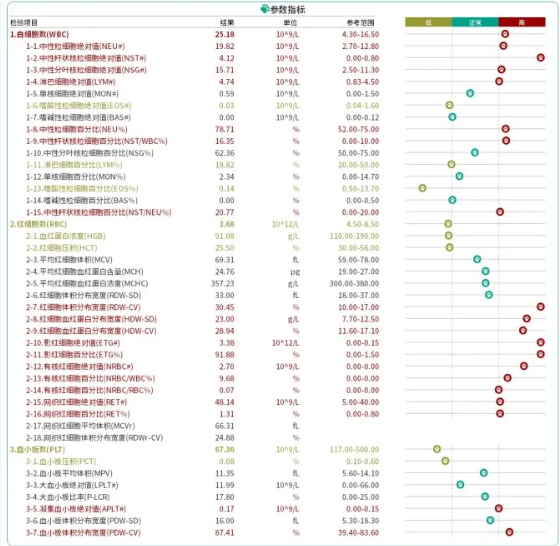
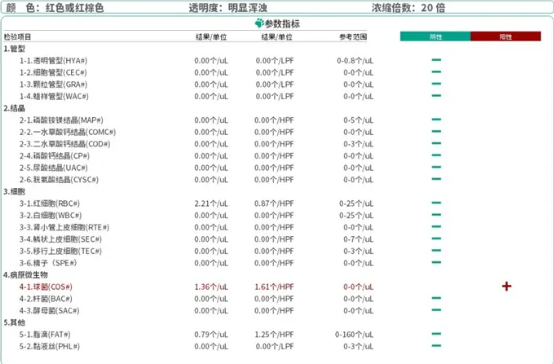
2.2 Anlu Formed Components Blood Analysis
The results of Anlu's blood formed elements indicated a severe inflammatory state in the animal, with a left shift in nuclei and high lymphocyte count; the erythrocyte count indicated a regenerative anemia in the animal, with a large number of nucleated erythrocytes released from the bone marrow and a large number of shadow erythrocytes.
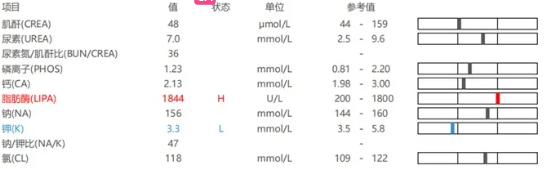
2.3 Biochemical Analysis
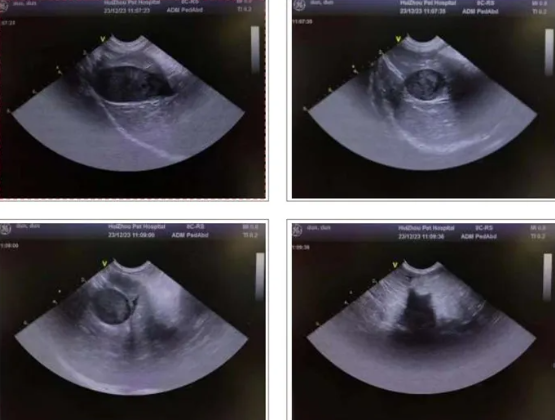
2.4 Ultrasound examination
1. The gallbladder wall is smooth, with unclear internal echoes, and no obvious dilation of the bile duct is observed.
2. The liver is normal in shape and size, with a smooth and continuous capsule, homogeneous parenchymal echogenicity, and clear intrahepatic tubular structures with normal course. Hypoechoic areas are visible in the interlobular spaces of the liver.
3. The spleen is normal in shape but enlarged in size, with homogeneous parenchymal echoes and a slightly hypoechoic mass visible within it.
4. The size and shape of the duodenal bulb, descending segment, and horizontal segment are normal, and the walls are still smooth. No definite ulcers or masses are seen in any part of the duodenum, and there are no signs of duodenal reflux.
5. Both kidneys are normal in size and shape, with smooth and regular contours, homogeneous parenchymal echoes, no space-occupying lesions, no separation of the collecting system, no dilation of either ureter, and no obvious abnormal echoes within them. The bladder is adequately filled, with smooth and continuous walls, and no obvious abnormal echoes within the cavity. A fluid-filled dark area is visible around the bladder.
2.5 Anlu Formed Components Urine Analysis
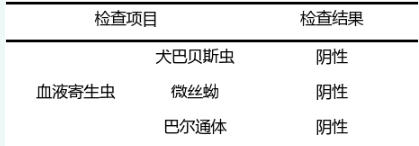
2.6 Blood smear
03 Preliminary diagnosis
Jaundice can be classified into prehepatic jaundice, hepatic jaundice, and posthepatic jaundice based on the location of the lesion.
Based on imaging results and urinalysis of formed elements, the dog did not have urinary system disease . Biochemical and liver ultrasound results ruled out hepatic jaundice. Gallbladder ultrasound ruled out post-hepatic jaundice, suggesting pre-hepatic jaundice. A mass was found on spleen ultrasound; blood smear screening showed no blood parasites; and treatment with blood transfusions and hormones was ineffective. Through a process of elimination, the diagnosis was directed towards IMHA (intracytoplasmic liver disease).
A definitive diagnosis requires a combination of hemagglutination tests or Coombs tests. It is not yet clear whether the animal has primary or tumor-related IMHA, but it has already provided guidance for clinical treatment.
04 Treatment strategies for IMHA
Treatment for IMHA depends on the specific condition of the animal and may require intervention to control the inflammatory response. This includes using antibiotics to control the infection and reduce the severity of the inflammation.
At the same time, it is necessary to determine whether IMHA is primary or secondary. If it is secondary, the underlying disease needs to be considered, and immunosuppressive therapy may be necessary. If it is primary, the immune response needs to be controlled, which may require the use of hormones or other medications.
The treatment approach can be summarized as follows:
4.1 Blood Transfusion Therapy
The decision to administer blood transfusions should take into account the animal’s anemia, including blood test results (such as HCT, RBC, HGB, etc.), the severity of clinical symptoms, resting blood lactate concentration, and the rate of anemia progression.
For animals in urgent need of red blood cells, immediate transfusion should be administered. Fresh packed red blood cells are recommended when the animal exhibits clinical signs of reduced oxygenation. If packed red blood cells are unavailable, whole blood transfusion can be considered, but fresh frozen plasma is not recommended for dogs with IMHA. Furthermore, the impact of autoagglutination on crossmatching and blood typing results needs to be considered.
In this case, the dog had already received a blood transfusion.
4.2 Immunosuppressive therapy
Immunosuppressive therapy plays a central role in the treatment of IMHA, primarily by using non-specific immunosuppressants, such as glucocorticoids, to suppress the autoimmune response against erythrocyte antigens.
However, immunosuppressive therapy is often accompanied by numerous adverse reactions, especially related to the type of drug and the duration of treatment. In severe cases (usually due to ineffective immunosuppressants) or relapses after IMHA recovery, second-line drugs such as azathioprine, cyclosporine, and mycophenolate mofetil are sometimes considered as routine treatment for IMHA dogs to enhance the immunosuppressive effect of the drugs, achieve faster initial disease control, and gradually reduce the use of glucocorticoids.
4.3 Inhibition of thrombus formation
The second important aspect of canine IMHA treatment is the inhibition of thrombus formation, particularly pulmonary thromboembolism, which is a major cause of morbidity and mortality.
This is achieved by using antiplatelet and anticoagulant drugs, which inhibit platelet function and coagulation factor activity, respectively. ACVIM recommends thrombosis prophylaxis for all dogs with IMHA, but for dogs with platelet counts below 30,000/μL, anticoagulant injections may not be chosen because the use of antiplatelet drugs may increase the risk of spontaneous bleeding.
In this case, the dog's platelet count was below the reference value, and no anticoagulant was administered.
05 Analysis and Discussion
5.1 Etiology of IMHA
IMHA is an antibody-mediated cytotoxic (type II) immune response. Its pathogenesis involves autoantibodies or complement attaching to the surface of red blood cells, leading to red blood cell rupture.
Immune-mediated hemolytic anemia (IMHA) can be classified into primary and secondary types. In dogs, IMHA is usually primary, while it is more common in cats to be secondary.
Primary IMHA is caused by antibody binding to an unchanged intrinsic erythrocyte membrane antigen. IMHA is triggered when the autoantigen is recognized and destroyed by the immune system. Primary IMHA includes autoimmune diseases such as lupus, as well as breed-specific genetic disorders such as those in Cocker Spaniels, Schnauzers, Collies, English Sheepdogs, Maltese, Poodles, and Irish Setters.
Secondary IMHA is associated with factors such as feline leukemia, blood parasites, drugs, vaccines, and tumors [2,3] .
5.2 IMHA Diagnosis
The ACVIM consensus statement on the diagnosis of IMHA in dogs and cats states that to confirm IMHA, at least the following conditions must be met: at least two markers of immune-mediated destruction (such as positive slide agglutination, positive DAT, or spherocytes), and at least one marker of hemolysis (such as jaundice/hyperbilirubinemia/significant bilirubinuria, hemoglobinemia/hemoglobinuria, or shadow cells), and other obvious causes of anemia must be excluded.
In this case, blood analysis of the formed elements revealed spherocytes, erythrocytes, and unexplained regenerative anemia in the animal. These findings led clinicians to suspect IMHA.
Shadow erythrocytes are formed when red blood cells rupture, causing hemoglobin to leak out, and then the red blood cell membrane closes again due to surface tension. Shadow erythrocytes are a marker of intravascular hemolysis. Anlu's blood testing module can perform absolute quantification of shadow erythrocytes, thereby assessing the degree of intravascular hemolysis in animals.
In this case, Anlu's formed element blood analysis can also perform absolute quantification of reticulocytes and nucleated erythrocytes, thus fully assessing the regeneration of erythrocytes in the animal. An increase in the number of reticulocytes and nucleated erythrocytes was observed in the animal, suggesting that although the animal had anemia, its bone marrow had a strong capacity for erythrocyte regeneration.
When the body is in a state of severe anemia, severe hypoxia occurs, leading to increased erythropoietin synthesis and active erythroid proliferation. This causes compensatory erythrocyte synthesis, resulting in the release of some nucleated erythrocytes into the peripheral blood. Detecting nucleated erythrocytes (NRBCs) in peripheral blood can be used to determine the degree of anemia and hypoxia, helping to assess the cause and progression of anemia. These findings provide a clear indication for the diagnosis of IMHA.
06 References
1. Swann JW, Garden OA, Fellman CL, et al.AACVIM consensus statement on the treatment of immune-mediated hemolytic anemia in dogs.[J] Vet Intern Med.2019,33(3):1141-1172. doi:10.1111/jvim.15463
2. AR Klag , U Giger , FS Shofer .Idiopathic immune-mediated hemolytic anemia in dogs: 42 cases (1986-1990).[J].Am Vet Med Assoc,1993, 202(5):783-8
3. MILLER SA, HOHENHAUS AE, HALE A S. Case-control study of blood type, breed, sex, and bacteremia in dogs with immune-mediated hemolytic anemia.[J]. Am Vet Med Assoc, 2004, 224(2): 232-5.